Will Cranking Machines Eith a Jerk Cord Hurt the Baby
Disabled Village Children
A guide for community health workers,
rehabilitation workers, and families
Part i
WORKING WITH THE CHILD AND FAMILY:
Information on unlike Disabilities
B. Recognizing, Helping with, and Preventing Common Disabilities
059
Affiliate 7
Polio
Infantile Paralysis
HOW TO RECOGNIZE PARALYSIS Acquired By POLIO
-
Paralysis (musculus weakness) usually begins when the kid is small, often during an illness similar a bad cold with fever and sometimes diarrhea.
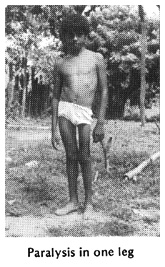
- Paralysis may bear upon whatsoever muscles of the body, merely is most common in the legs. Muscles most often affected are shown in the drawing.
- Paralysis is of the 'floppy' blazon (not strong). Some muscles may exist but partly weakened, others limp or floppy.
- In fourth dimension the affected limb may not be able to straighten all the way, due to shortening, or 'contractures', of certain muscles.
- The muscles and bones of the affected limb become thinner than the other limb. The affected limb does non abound every bit fast, and so is shorter.
- Unaffected arms or legs often become actress strong to brand up for parts that are weak.
- Intelligence and the mind are not affected.
- Feeling is not affected.
-

'Articulatio genus jerks' and other tendon reflexes in the affected limb are reduced or absent-minded. (In cerebral palsy, 'knee jerks' frequently bound more normal. See Page 88.) As well, the paralysis of polio is 'floppy'; limbs affected past cerebral palsy often are tense and resist when straightened or bent (meet Page 102).
- The paralysis does not get worse with time. Notwithstanding, secondary problems like contractures, curve of the backbone and dislocations may occur.
| Of children who become paralyzed by polio: | |||
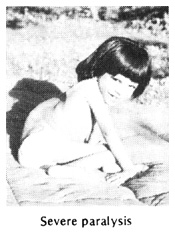
| 30% recover completely in the first weeks or months.  | 30% take mild paralysis.  | 30% have moderate or astringent paralysis.  | 10% die (ofttimes because of difficulty animate or swallowing).  |
060
BASIC QUESTIONS AND ANSWERS Nigh POLIO
How mutual is it? In many countries, polio - or 'poliomyelitis'- is still the most common cause of physical inability in children. In some areas, at least one of every 100 children may have some paralysis from polio. Where vaccination programs are constructive, polio has been greatly reduced.
What causes it? A virus (infection). The infection attacks parts of the spinal string, where it amercement only the fretfulness that command motion. In areas with poor hygiene and lack of latrines, the polio infection spreads when the stool (shit) of a sick child reaches the oral fissure of a salubrious child. Where sanitation is better, polio spreads mostly through coughing and sneezing.
Practice all children who become infected with the polio virus become paralyzed? No, only a minor per centum get paralyzed. Nigh only get what looks similar a bad cold, with fever. However, if a kid with a 'cold' caused past the polio virus is given an injection of any medication, the irritation acquired past the injection can bring on paralysis. (Encounter warning on Page 19.)
Is the paralysis contagious? No, not subsequently 2 weeks from when a kid showtime gets sick with polio. In fact, most polio is spread through the stool of non-paralyzed children who have 'just a cold' caused by the polio virus.
At what age exercise children become polio? In areas with poor sanitation, polio near often attacks babies from eight to 24 months one-time, but occasionally children up to age 4 or 5. Every bit sanitation improves, polio tends to strike older children and even young adults.
Who does it most frequently affect? Boys, a piddling more than than girls. Unvaccinated children much more often than vaccinated children. (See Page 74). Immature children who are given injections unnecessarily are paralyzed by polio more often those who are not.
How does the paralysis begin? It begins later signs of a common cold and fever, sometimes with diarrhea or airsickness. Later on a few days the neck becomes stiff and painful and parts of the trunk get limp. Parents may find the weakness right away, or only subsequently the kid recovers from the acute disease.
Once a child is paralyzed, what changes or improvements can be expected? Ofttimes the paralysis will gradually go away, partly or completely. Whatever paralysis left after 7 months is commonly permanent. The paralysis will not get worse. However, certain secondary problems may develop-especially if precautions are non taken to prevent them.
What are the child's chances of leading a happy, productive life? Commonly very good-provided the kid is encouraged to do things for himself, to become the most out of school, and to larn useful skills inside his concrete limitations (encounter Page 497).
Can persons with polio ally and have normal children? Yep. Polio is non inherited (familial) and does not bear upon ability to accept children.
061
SECONDARY Bug TO Expect FOR WITH POLIO
By secondary problems, nosotros mean further disabilities or complications that can announced after, and considering of, the original disability.
CONTRACTURES OF JOINTS
A contracture is a shortening of muscles and tendons (cords) so that the full range of limb motion is prevented.
Unless preventive steps are taken, joint contractures will form in many paralyzed children. In one case formed, oftentimes they must be corrected before braces can exist fitted and walking is possible. Correction of advanced contractures, whether through exercises, casts, or surgery (or a combination), is costly, takes fourth dimension and causes discomfort. Therefore early prevention of contractures is very of import.
A total discussion of contractures, their causes, prevention, and treatment is in the adjacent chapter (Chapter 8). Methods and aids for correcting contractures are described in Chapter 59.
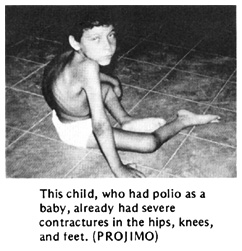
TYPICAL CONTRACTURES IN POLIO
A child with paralysis who crawls around like this rid never straightens her legs volition gradually develop contractures so that her hips, knees, and ankles tin can no longer be straightened.
OTHER Mutual DEFORMITIES
Weight bearing (supporting the body's weight) on weak joints tin can cause deformities, Including:
| OVER-STRETCHED JOINTS | DISLOCATIONS |
| | |
SPINAL Bend
| Minor curve of spine can be caused by tilted hips, as a result of a curt leg. |  | More serious curve of the spine is caused by muscle weakness of the back or body muscles. The curve can go and then severe that it endangers life by leaving too piddling room for the lungs and center. |  | At showtime, the spinal bend straightens when the kid is positioned improve. But in time the curve becomes more fixed (will not straighten any more). For information on spinal curves, come across Chapter 20. |
062
WHAT OTHER DISABILITIES CAN BE Dislocated WITH POLIO?
- Sometimes cerebral palsy tin can be mistaken for polio-especially cerebral palsy of the 'floppy' type.
| Nevertheless, cognitive palsy unremarkably affects the body in typical patterns: | Polio has a more irregular blueprint of paralysis. |
 |  |
In cerebral palsy, usually you can observe other signs of brain damage: over-agile knee jerks and abnormal reflexes (see Page 88), developmental delay, awkward or uncontrolled motion, or at least some muscle tenseness (spasticity).

- In muscular dystrophy, paralysis begins little by little and steadily gets worse (meet Folio 109).

-
Hip issues (meet Page 155) can cause limping, and muscles may become thin and weak. Cheque hips for pain or dislocations. (Note: Confused hip may also occur secondary to polio.)
Note: Polio tin occur before or subsequently a child has whatever of these other problems. Check carefully.

-
Clubbed foot is nowadays from birth (meet Page 114).

-
'Erb'southward palsy', or partial paralysis in one arm and hand, comes from birth injury to the shoulder (see Page 127).

-
Leprosy. Foot and hand paralysis begins gradually in older child. Often there are peel patches and loss of feeling (see Page 215).

-
Spina bifida is present from nascence. In that location is reduced feeling in the feet, and often a lump (or scar from surgery) on the back (see Page 167).
Always EXAMINE THE Dorsum IN A CHILD WITH PARALYSIS OF THE LEGS, AND Bank check FOR FEELING.

-
Injuries to the spinal cord (see Page 175) or to particular nerves going to the artillery or legs. In that location is usually a history of a severe back or neck injury, and loss of feeling in the paralyzed role.

-
Tuberculosis of the spine can cause gradual or suddenly increasing paralysis of the lower body. Look for typical crash-land on spine (run into Page 165).
- Other causes of paralysis or muscle weakness. There are many causes of floppy paralysis like to polio. I of the most mutual is 'Guillain-Barre' paralysis. This tin can outcome from a virus infection, from poisoning, or from unknown causes. Information technology commonly begins without alert in the legs, and may spread within a few days to paralyze the whole torso. Sometimes feeling is too reduced. Ordinarily force slowly returns, partly or completely, in several weeks or months. Rehabilitation and prevention of secondary problems are basically the same every bit for polio.
063
WHAT Can Exist DONE?
DURING THE ORIGINAL Illness, when the kid get-go becomes paralyzed:
-
No medicines aid, either during the first illness, or later.
-
Residue is important. Avoid forceful practice because this may increment paralysis. Avoid injections.
-
Good nutrient during recovery helps the child go stronger. (But take care that the child does non eat besides much and become fat. An overweight child will accept more than problems with walking and other movements.) For suggestions about skillful food, encounter Where There Is No Doctor, Chapter 11.
-
Position the child to be comfortable and to avoid contractures. At beginning the muscles will be painful, and the child will not want to straighten his joints. Slowly and gently try to straighten his arms and legs so that the child lies in asgood a position as possible. (See Chapter eight.)
| Skilful POSITION Artillery, hips, and legs as straight equally possible. Feet supported. | BAD POSITION Bent arms, hips, and legs. Feet in tiptoe position. |


Note: To reduce pain, you may demand to put cushions under the knees, merely try to go along the knees every bit directly every bit you can.
FOLLOWING THE ORIGINAL Disease:
-
Continue with proficient food and good positions.
-
As before long as the fever drops, commencement exercises to forbid contractures and render forcefulness. Range-of-movement exercises are described in Chapter 42. Whenever possible, brand exercises fun. Active games, swimming, and other activities to keep limbs moving as much equally they tin can are important throughout the child'due south rehabilitation.
-
Crutches, leg braces (calipers), and other aids may help the child to motion better and may foreclose contractures or deformities.
-
In special cases, surgery may exist needed to correct contractures, or to change the place where strong muscles attach, so that they help do the work of weak ones. When a human foot is very floppy or bends to one side, surgery to bring together certain bones of the foot may aid. But considering bone surgery stops the growth of the foot, ordinarily it should not be washed before age 12 or thirteen.
-
Encourage the kid to use his body and mind as much every bit possible, to play actively with other children, to take care of his daily needs, to help with work, and to become to school. As much as possible, treat him similar any other child.
064
REHABILITATION OF THE Kid WITH PARALYSIS

All children paralyzed by polio tin can be helped past sure basic rehabilitation measures-such every bit exercise to continue a full range of motion in the afflicted limbs.
Nonetheless, each child will have a different combination and severity of paralyzed muscles, and therefore will have his own special needs.
For some children, normal do and play may be all that are needed. Others may require special exercises and playthings. Still others may need braces or other aids to assistance them motility about better, do things more easily, or keep their bodies in healthier, more than useful positions. Those who are severely paralyzed may be helped most by a wheelboard (trolley) or wheelchair.
Every kid needs to be advisedly examined and evaluated in social club to all-time meet his or her item needs. The before you evaluate a kid'southward needs, and take steps to meet them, the better.
Unfortunately, 'in most areas where polio is still common, village rehabilitation programs do non be or are just beginning. Many children (and adults) who take been paralyzed for a long fourth dimension already have astringent deformities or articulation contractures. Frequently these must be corrected before a child tin can use braces or begin to walk.
Because contractures are such a mutual problem, non simply with polio but with many other disabilities, we discuss them separately in the next chapter. Before evaluating a child with polio, we strongly suggest you read Chapter viii on contractures.
WARNING: Before deciding on any assist or procedure, carefully consider its advantages and disadvantages. For example, some deformities may be best left uncorrected considering they actually help the paralyzed child stand straighter or walk better (see Page 530). And some aids or braces may prevent a kid from developing strength to walk without aids (see Page 526).Before deciding what aid or procedure to utilise, we suggest you lot read Affiliate 56, "Making Certain Aids and Procedures Exercise More Good Than Harm."
065
PROGRESS OF A Child WITH POLIO:
THE Changing NEEDS FOR AIDS AND ASSISTANCE

1. exercises to keep full range of motion, starting within days later on paralysis appears and continuing throughout rehabilitation

2. supported sitting in positions that assist prevent contractures

three. active exercises with limbs supported, to proceeds strength and maintain total motility
four. exercise in water - walking, floating, and swimming, with the weight of the limbs supported past the h2o

5. wheelboard or wheelchair with supports to prevent or right early on contractures.

Notation: These also provide good arm exercise in preparation for walking with crutches.

6. braces to preclude contractures and prepare for walking

7. parallel bars for first to balance and walk

8. walking machine or 'walker'

9. crutches modified every bit walker for balance and extra support

x. under arm crutches

xi . forearm crutches and perhaps in time . . .

12. a pikestaff or no arm supports at all
Note: These pictures are merely an instance - but most of the steps are necessary for many children. Children who begin rehabilitation late may also have contractures or deformities requiring corrective steps not shown here.
066
EVALUATING A Kid'Due south NEEDS FOR AIDS AND PROCEDURES
Step 1: Outset by learning what you can through talking with the child and family unit (meet Kid's History, Page 37 to 38). As you do this, sentry the child move about. Observe advisedly which parts of the body seem potent, and which seem weak. Look for whatever differences betwixt one side of the body and the other-such as differences in the length or thickness of the legs. Are there whatever obvious deformities, or joints that do not seem to straighten all the style? If the child walks, what is unusual about the manner she does it? Does she dip forward or to one side? Does she assist support one leg with her manus? Is one hip lower than the other? Or i shoulder? Does she have a humpback, a swayback, or a sideways curve of the back?
These early observations will help you know what parts of the body y'all about need to check for strength and range of motion. Often, by watching a kid you lot can begin to go an idea about what kind of aids or assistance may assistance. For example:
 Carmen appears to accept severe paralysis affecting both legs and her correct arm. Weakness in her trunk (master part of the body) appears to take acquired a severe S-shaped curve of the spine. |  She will probably never walk, and will need a wheelchair or wheelboard. You lot may want too to brand her a body brace, or assistance her in other ways to sit down more upright and try to keep the spine from angle more than. |

Pedro appears to accept severe paralysis in his legs and hips. It looks as if his hips, knees, and feet cannot straighten (contractures). Weak stomach muscles and astringent hip contractures may be the crusade of his swayback.
Because his artillery look stiff, Pedro will probably be able to walk with crutches and leg braces. Only showtime his contractures must be straightened.
If the contractures cannot be straightened past gradual stretching, he may need surgery.
067
Manuel walks with the assist of a stick. He appears to take paralysis mainly in his right leg and pes. Because of weak thigh muscles, he 'locks' his human knee backward in order to comport weight on it. This 'dorsum-kneeing' has go more and more than farthermost as the cords behind the human knee stretch. The foot is very unstable and flops to i side. The weaker leg looks somewhat shorter-and for walking is much shorter because of the bent-back knee and bent-over human foot.

He might be able to walk without the stick if he uses a beneath-knee joint brace to stabilize his pes. (Run across Page 550.)
Simply the back-genu would become worse and worse until he could not walk. So probably he should take a long-leg brace. The brace might allow his human knee to bend backward just a niggling for stability - and so that no knee joint lock is needed.

Afia leans forrard and pushes her weak left thigh with her mitt when she walks. Her left knee cannot quite straighten. Her weak leg looks a picayune shorter than the other.
Exercises to become her knee straighter or so it can bend very slightly astern may be all that is needed for Afia to walk without using her paw.

Or she may demand an to a higher place-knee caryatid with a strap to pull the knee dorsum.
Or she may just need a below-knee brace that helps push her knee dorsum.
The brace bends the human foot down just a little, so that past bearing weight on toes (rather than heel) her knee is pushed back.
To get a better thought well-nigh which of the three solutions may work all-time for Afia, you will demand to do a careful physical test, testing range of move and muscle force of the hip, knee, and ankle joints.
Step. 2: This is the physical examination. Information technology should unremarkably include:
1.Range-of-motility testing, particularly where you call back in that location might exist contractures. (See "Physical Examination," Page 27 to 29, and "Contractures," Page 79 and 80.)
2. Muscle testing, especially of muscles that you call back may be weak. Likewise examination muscles that need to be potent to brand up for weak ones (such as arm and shoulder strength for crutch use). (See Page 27 and Page 30 to 33.)
3. Check for deformities: contractures; dislocations (hip, knee, pes, shoulder, elbow); difference in leg length; tilt of hips; and bend or abnormal shape of the back. (See Page 34.)
068
Step three: After the concrete exam, again observe how the child moves or walks. Endeavor to relate her particular way of moving and walking with your physical findings (such as weakness of sure muscles, contractures, and leg length). (For an example, see Folio 70.)
Step 4: Based on your observations and tests, effort to effigy out what kind of exercises, aids, or assistance might help the child nigh. Consider the advantages of different possibilities: benefit, cost, comfort, advent, availability of materials, and whether the kid is likely to apply the aid you brand. Ask the child and parents for their opinions and suggestions.
Pace 5: Earlier making a terminal brace or aid to fit the child, if possible test to see how well it may piece of work by using a temporary aid or one-time brace from another kid. For example,
 If a child'south ankle bends over to the exterior similar this... |
 ...a elevator on the outer side of the sole similar this, may help to keep the foot straighter. |
 Merely before nailing and glueing in the lift, speedily make a trial one of cardboard or something else and fasten it temporarily to the sandal or shoe with tape or string. So take the child walk. Note: For a few children, a lift similar this will assistance. For many it volition not. |
Ask the kid what she thinks.
Pace 6: After the kid, her parents, and you have decided what kind of brace or assist might work all-time, take the necessary measurements and make the brace or aid. When making it, once once more it is wise to put information technology together temporarily so that you tin can brand adjustments before y'all rivet, glue, or nail it into its concluding form. (See Page 540.)
Step vii: Have the child endeavor the brace or aid for a few days to get used to information technology and to see how well it works. Ask the child and parents if it seems to help. Does it hurt? Are there any problems? How could information technology be improved? Is in that location something that might work amend? Make what adjustments are necessary. Just remember that no brace or aid is likely to meet the needs of a child perfectly. Practise the best yous tin can.
069
Here is a story of how workers in a small village rehabilitation program figured out what kind of aids a child needed. How many of the steps we have just discussed did they follow? Was each step important?
A STORY: A Brace FOR SAUL
1 twenty-four hours a mother from a neighboring village arrived at the village middle with her six year onetime son, Saul. Mari and Chelo, 2 of the village rehabilitation workers, welcomed them warmly. Learning that Saul had polio equally a baby, they asked him to walk, and then to run, while they watched carefully. Saul limped a lot and i leg looked thinner and shorter. With each step it aptitude dorsum at the knee.
"He walks quite well, really," said Mari. "Just he has to 'lock' his knee joint back in order to put weight on it. That knee is going to keep stretching back and some day it will give out."
"A long-leg brace would protect his knee joint," suggested Chelo.
"Oh, please, no!" said Saul's mother. "A twelvemonth ago nosotros took Saul to the city and the doctors had a big metal caryatid made for him. It toll so much nosotros are still in debt! Saul hated it! He would always take it off and hide information technology. We tried and tried to get him to use it, but he wouldn't."

"That's not surprising," said Mari. "Oftentimes a kid who can walk without a caryatid volition refuse to apply one-fifty-fifty if he walks better with information technology. We could make him a long-leg brace out of plastic. It would be much lighter. What practice you lot say, Saul?" Saul began to cry.
"Don't worry, Saul. Peradventure we can do something simpler," said Mari. "But first let's examine you, okay?" Saul nodded.
On muscle testing Saul, they found he could not straighten his knee at all. But he had off-white force for angle his knee back

and his hip forward,
and good forcefulness for bending his hip dorsum.
070
"With the hip and thigh forcefulness he has, he should virtually be able to stand on that leg without the knee joint angle back," said Mari. "Saul, let's encounter you try it like this. Pretend you lot're a stork!" For a moment Saul could do it. "Good!" said Mari. "Every day stand like that and see how high you can count without letting your knee become dorsum. Every solar day try to crush your sometime tape! Okay?"
"Okay," said Saul. Sounds like fun!"
"The stork exercises may help," said Chelo. "But I nevertheless think he needs a brace. At to the lowest degree at outset."
We must weigh the advantages against the disadvantages," said Mari. "A long-leg caryatid would keep his knee joint straight. Simply it could weaken the muscles he needs to strengthen. Since the brace would continue his leg from bending dorsum, he wouldn't have to use his muscles to do it.
"On the other hand, we might try a short-leg brace that holds his foot at nearly a right angle. Then, to step apartment he volition have to keep his human knee nearly directly. It could help him strengthen his behind-the-thigh muscles."
"Let'due south try it!" Everyone agreed, except Saul.

Chelo brought someone's old, lower-leg plastic brace and showed it to Saul. "See how it will fit correct effectually your leg. It isn't heavy at all. Lift information technology! And no metal joints to go far the manner! What practise you lot say? Practice you lot want to try it?"
"I approximate and then," said Saul.
When the brace was made, they tested information technology. Saul said he liked information technology. At first, when he tried hard, he could walk without bending his knee back. But later on a few days, his mother complained that often he would walk, or even stand, with his knee bent fashion back as before, and his toes in the air, similar this.


"I have an idea," said Chelo. "Why don't we let the heel stick out behind the shoe. That way, when he steps, his weight will come well forward of the back of his heel. This should help bring his pes down and his knee frontward."
They tried information technology, and nearly of the time (especially when he was reminded) Saul walked without letting his human knee curve back much."

At habitation Saul's mother encouraged him to practise his stork exercises. As his muscles grew stronger, he began to walk without angle his knee far back-even in active play!
071
WILL MY Kid EVER BE ABLE TO WALK? "

This is often i of the first questions asked by the parents of a disabled child. It is an of import question. However, we must help parents realize that other things in life can be more important than walking (run across Page 93).
If the child whose legs are severely paralyzed by polio is to walk, mostly she volition need at least 2 things:
1. fairly strong shoulders and arms for crutch use
2. fairly direct legs (hips, knees, and feet). (it is important to correct contractures so that the legs are straight or almost straight before trying to suit braces for walking.)
To evaluate a child's possibility for walking, always test arm and shoulder strength:
Have her attempt to lift her body weight off the footing with her artillery, like this.
If she can hands lift upwards and downwardly several times, she has a Skilful run a risk of beingness able to walk using crutches.
If her arms and shoulders are and so weak she cannot brainstorm to lift herself, her chances for crutch - walking are POOR.

If her shoulder and arm strength is FAIR, and the child tin almost lift herself, daily exercise lifting her weight like this may increment strength enough to make crutch utilize possible.
Having the child lift herself while holding bar like this volition also aid strengthen her easily and wrists for crutch use.

Pushing herself in a wheelchair or wheelboard (trolley) is a practical way to strengthen shoulders, artillery, and hands.

If the child cannot elevator herself because of weak elbows, put simple splints on her arms to meet if she can lift herself with these.

If she can elevator herself with the elbow splints, mayhap she can use crutches that give elbow support.

If she is fat, she should lose weight. This volition brand walking on weak limbs much easier.
Now bank check how directly the legs volition go. (See range-of-motion testing, Page 27.)

If the hips, knees, and feet can be placed in adequately straight positions, chances for walking soon with braces are practiced (if arm strength is good).
But if the child has much contracture of the hips, knees, or feet, these will demand to be straightened before she will be able to walk.
For correction of contractures, run across Chapters 8 and 59.

Sometimes, if contractures are severe in ane leg only, the child tin can learn to walk on the other leg merely, with crutches. Only information technology is best with both legs, whenever possible.
072
Afterward checking arm strength and leg straightness, the next thing to check is the force in the ankles, knees, and hips. This volition assist yous make up one's mind if the child needs braces, and what kind.
A kid with a foot that hangs down (foot drop), or flops to one side may be helped by a below-knee caryatid of plastic or metal.
For foot drop, you can make a brace that lifts the foot with a jump or rubber band. (See Page 545.)
The kind of brace you choose will depend on various factors, including price, available skills and materials, and what seems to work all-time for the item child. Advantages and disadvantages of different kinds of braces, and how to brand them, are discussed in Affiliate 58.
A child with a weak knee may need a long-leg brace of plastic or metal.
Note: Not all children with no strength to straighten the knee joint need long-leg braces:A child with stiff butt muscles may be able to walk without a caryatid.

If a child has a contracture and cannot walk with his articulatio genus direct, correcting the contracture until his genu bends very slightly backward may allow him to walk better.

Caution: A stiff human foot with a moderate tiptoe contracture may help push the knee dorsum, merely like a stiff brace. Correcting the contracture may brand walking more than difficult or impossible, so that a brace is needed where none was needed earlier. (See Chapter 56.)
073
A kid with very weak hip muscles may discover his leg flops or twists about besides much with a long-leg brace.
He may demand a brace with a hip band to help stabilize the leg at the hip.
A child with weak body and back muscles, who cannot hold up her torso well, may need long-leg braces attached to a body caryatid or body jacket.

Note: Ofttimes a child at offset may need a hip band or trunk jacket to help stabilize her for walking. A few weeks or months later she may no longer need it. Removing it may help the kid gain more than strength and command. It is important to re-evaluate the child's needs for bracing periodically.
Have care to apply no more than bracing than is needed.
A kid whose courage is becoming seriously curved may do good from a body brace (or in severe cases, she may need surgery).

If necessary, the body brace can exist attached to long-leg braces as shown higher up.
More information on spinal curve can be establish in Affiliate 20. For information on how to make body braces and jackets, come across Affiliate 58.
074
PREVENTION OF POLIO

POLIO VACCINE, the all-time protection - IF it has been kept cold continuously!
-
Vaccinate babies with polio vaccine. Be sure they go the vaccine 3 times by the time they are 8 months one-time. It is usually best to give the offset polio vaccination around 3 months of age.
-
Vaccinate equally many children as possible. The vaccine given by oral cavity is alive. So, if most of the children are vaccinated, the alive vaccine volition spread to children who take not been vaccinated, and protect them too.
-
Try to Keep the live polio vaccine frozen until shortly before it is used. For upwardly to iii months it tin be thawed and refrozen. Only it must be kept cold or it will spoil.

-
Seek community help with vaccination and in keeping vaccine common cold. Sometimes vaccines do not reach villages because health posts lack refrigeration. Merely ofttimes shop-keepers and a few families have refrigerators. Win their interest and cooperation.
-
To give best protection, vaccinate the child when she does not have a fever or a cold or diarrhea. But if by 6 months of age, the kid still has non been vaccinated, requite her the polio vaccine even if she is a picayune sick. However, in that location is a chance that the vaccine may not work if it is given when the kid is sick (with a virus infection). Therefore, still try to give the complete series of three vaccinations and one booster later, when the kid is non sick.
It is estimated that in poor countries at least one-third of vaccines are spoiled past the fourth dimension they achieve the children. Therefore, fifty-fifty in children who have been vaccinated, boosted precautions are needed:

-
Breast feed your babe as long as possible. Breast milk contains 'antibodies' that may help protect against polio. (Babies rarely get polio before 8 months old because they still have their mothers' antibodies. Breast feeding may make this protection concluding longer.)
-
Do not give injections of any medicine to babies or children, except when absolutely necessary. Irritation acquired by injected medicine can turn a mild, undiagnosed polio infection into paralysis. It is estimated that today 1 out of 3 cases of paralysis from polio is brought on by injections (run across Page xix).
-
Organize the people and help out in popular campaigns to encourage vaccination, chest feeding, and express, sensible use of injections. Community theater and boob shows are good ways to raise sensation on these issues. Meet Chapter 48.
075
PREVENTION of secondary problems
We have already discussed some means to preclude new problems or complications in a child with paralysis. In summary, important measures include:
-
Prevent contractures and deformities. Brainstorm appropriate range-of-motion exercises every bit soon equally the paralysis appears.
-
At the starting time sign of a joint contracture, do stretching exercises 2 or 3 times a day- every day.
| Stretching exercises work ameliorate if you lot stretch the joint firmly and continuously for a few moments,  | instead of 'pumping' the limb back and forth.  We emphasize this indicate because in many countries parents are taught the pumping method - which does very little skilful. |
For more details, see "Contractures," Chapter 8.
-
Evaluate the kid's needs regularly, and change or suit aids, braces, and exercises to see her changing needs. Too little or too much bracing can concord the child back or create new problems.

- Be sure crutches do not press hard under the artillery; this tin cause paralysis of the hands (run across Page 393).
- Try non to let the kid's concrete disability concord back her overall physical, mental, and social evolution. Provide opportunities for her to pb an agile life and take function in games, activities, schoolhouse, and work with other children. PART two of this book discusses means to assistance the community meet the needs of disabled children.
OTHER PARTS OF THIS Volume THAT MAY BE USEFUL
IN MEETING NEEDS OF A CHILD Afflicted Past POLIO
* Specially important chapters are marked with a star:*
Physical examination, Affiliate 4
Measurement of contractures and progress, Chapter 5
* Contractures, Chapter 8
Dislocated hips, Chapter 18
Spinal curve, Chapter 20
* Range-of-movement and other exercises, Chapter 42
Crutch employ, wheelchair transfers, etc., Chapter 43
Community needs, social aligning, growing upward, Role 2, especially Chapters 47, 48, 52, 53
Making sure aids and procedures run into the child's needs, Chapter 56
* Braces and calipers, Chapter 58
* Correcting contractures, Chapter 59
Correcting club feet, Affiliate 60
Special seating and wheelchairs, Capacity 64, 65, 66
* Aids for walking, Chapter 63
For more than information on polio, see References Folio 637.
076
A Boy WITH POLIO BECOMES AN OUTSTANDING
HEALTH AND REHABILITATION WORKER
Marcelo Acevedo was disabled past polio. He and his family unit lived in a hamlet 2 days from the closest road. Village health workers from Project Piaxtla helped Marcelo go surgery for his human knee contractures. Afterwards surgery he got braces and went to school. Then they trained him as a village health worker, and he returned to serve his village.
When PROJIMO was formed, Marcelo joined as a village rehabilitation worker. He studied brace-making as an amateur in 2 caryatid shops in United mexican states City.
Marcelo is now one of the leaders in PROJIMO, and has gained the respect of the whole village. He has recently married a village woman.
Go dorsum to the CONTENTS
Disabled Village Children
A guide for customs health workers,
rehabilitation workers, and families
by David Werner
Published by
The Hesperian Foundation
P.O. Box 11577
Berkeley, CA 94712-2577
Source: https://www.dinf.ne.jp/doc/english/global/david/dwe002/dwe00209.html
{kind=link}
Post a Comment for "Will Cranking Machines Eith a Jerk Cord Hurt the Baby"